Normal Hip Anatomy
The hip is a ball-and-socket joint made up of the femur (ball) and acetabulum (socket) (Figure 1). Although the deep socket makes the hip inherently stable, it is further reinforced by a lining (capsule) and a ring of supporting fibrocartilage (labrum). All of these structures function together to allow for movement of the joint without conflict or instability (Figure 2A).
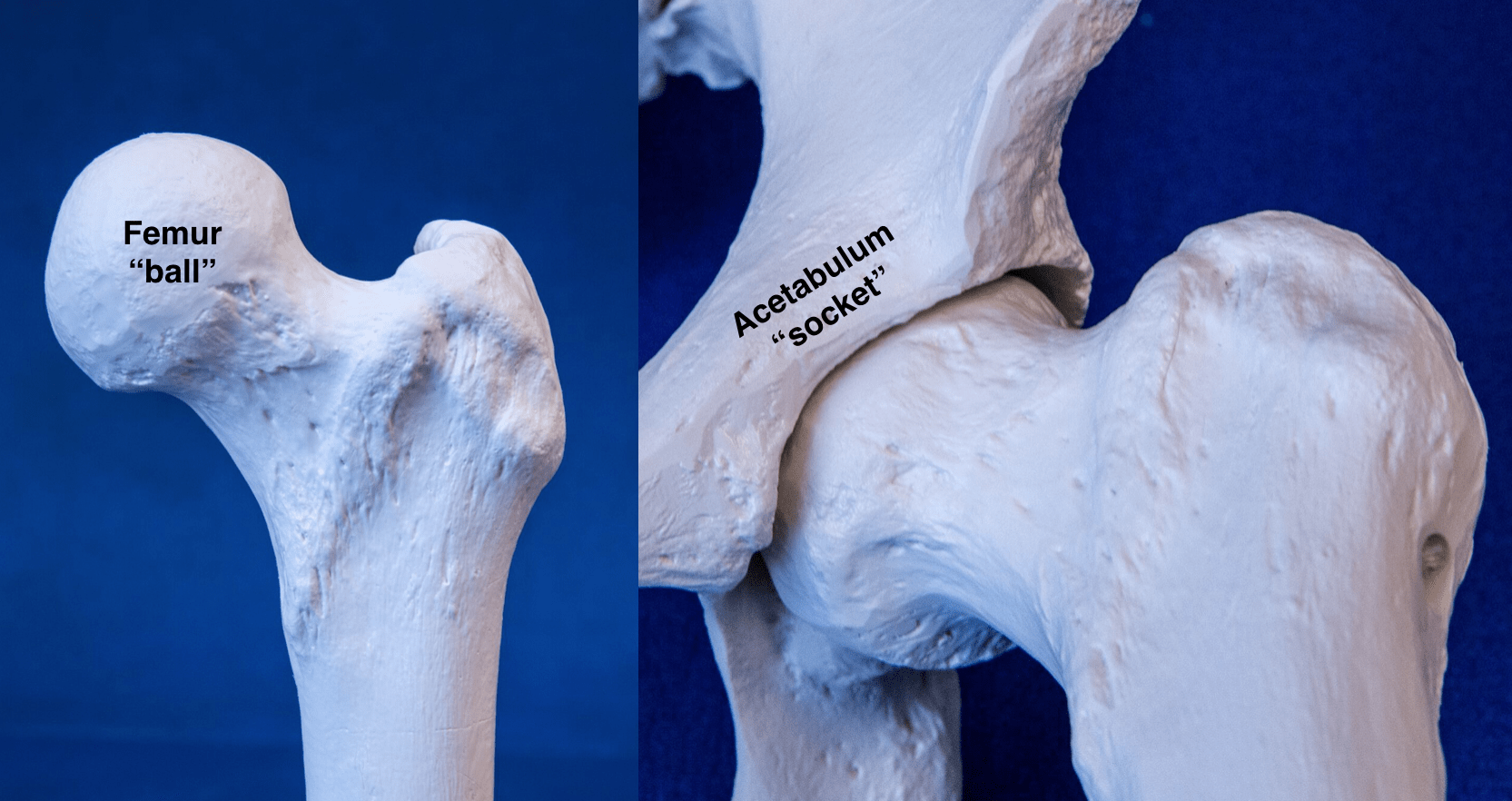
Figure 1 – Normal Hip Anatomy

Figure 2 – Normal vs Pathologic Hip Motion
What is acetabular dysplasia?
Acetabular dysplasia, or dysplasia, is a congenital disorder in which the hip socket is too shallow to adequately house the ball. Dysplasia is most commonly seen in females who have generalized ligamentous laxity allowing them to hyperextend their elbows, wrists, and knees. The shallow socket gives rise to hip instability, or excessive translational motion and increased shear forces within the joint. Typical anatomic abnormalities in acetabular dysplasia include:
- Shallow socket
- Enlarged labrum
- Ligamentous laxity or loose ligaments
- Excessive hip internal rotation or femoral antetorsion
What will happen if the dysplasia is left untreated?
The natural history of acetabular dysplasia is well documented and varies with the severity of dysplasia. Dysplasia is rated as either borderline or frank, with frank being the more severe variant. Patients with untreated frank dysplasia typically experience progressively worsening pain until the hip deteriorates to end-stage arthritis. Some studies have reported that the time to progress to severe arthritis may be as little as 5 years from the onset of symptoms. This makes frank dysplasia a semi-urgent condition for which time is of the essence. Delaying treatment may result in the accumulation of significant cartilage damage, which may then preclude a corrective osteotomy, making joint replacement the only viable option.
The natural history of borderline dysplasia is less clearly understood, and there is ongoing research in this area of hip preservation. Dr. Garabekyan approaches the treatment of borderline dysplasia on a case-by-case basis, incorporating the latest scientific evidence into his decision-making algorithm. Many borderline dysplastic patients may be adequately treated with minimally invasive arthroscopy alone, while some require a corrective re-alignment procedure. Dr. Garabekyan will discuss the important factors that enter into this complex algorithm, to achieve the best possible results.
What is the treatment for acetabular dysplasia?
The first line of treatment is conservative management, consisting of activity modification to avoid positions of instability, physical therapy to strengthen the surrounding musculature, and various injections to reduce inflammation and provide temporary relief. When these measures fail to provide adequate relief of symptoms, the next step is to surgically correct the underlying structural abnormality.
Surgery for dysplasia is tailored to each patient’s unique hip morphology to comprehensively address all sources of instability. A hip arthroscopy is first carried out to address any labral or cartilage tears, joint inflammation, and impingement. Following arthroscopy, patients may require a periacetabular osteotomy (PAO) and/or a derotational femoral osteotomy (DFO), depending on the unique pathomorphology. The second surgery is typically performed ~1 week following hip arthroscopy to allow for early rehabilitation to prevent scar tissue formation.
Am I a good candidate for periacetabular osteotomy (PAO) or derotational femoral osteotomy (DFO)?
Whether a re-alignment osteotomy (PAO or DFO) is a worthwhile option for you depends on a number of factors, including:
- Your age
- Your particular diagnosis or pattern of injury
- The extent of arthritis or cartilage damage
In general, the outcomes of realignment osteotomy are best in patients < 25 years of age with focal or discrete structural damage and minimal arthritis. Dr. Garabekyan will guide you through the various considerations in helping you decide whether re-alignment osteotomy is right for you.
Choosing the treatment option that is right for you involves careful consideration of your diagnosis, duration and severity of symptoms, desired level of activity, as well as social and financial elements. You are not alone in this process.
As you research your condition, please write down all of your questions and bring them with you to your next appointment. Dr. Garabekyan and his team at SCHI will take time to address all of your concerns, until you are completely satisfied with your treatment plan.
Related Topics: Labrum, Cartilage, Hip Arthroscopy, DFO, PAO



